I do not know how many people here have "Depression, Anxiety, Panic Disorders" but I am on disability for all three and it runs in my family on my mother's side.
So what is this article saying? Me and my family just do not have perseverance? That we lack the "will" not to be depressed and anxious? That I just need to "Aspir[e] toward personal and career goals"? HA!
No, it's not true. You see, they found we all have a genetic disorder (GCH1 Deficiency). After I yelled at my doctors for years to look more deeply they finally found that it was not that I did not have goals, but that I needed a low protein diet and some medications that a psychiatrist could not give me, and now I am doing better. Now I can have goals.
So while this article might be true for some people with situational depression, I hate these studies because people always said crap like this to me. I was "lazy" and just needed a hobby, and on and on. They psychiatric association does not recognize, still, that mood disorders can be caused by metabolic issues. When they say I do not have enough serotonin and I ask them why they looked at me like they were in Psych 101. And these articles make psychiatrists lazy, putting all the effort on the patient while they sit back and collect check after check.
I empathize with your frustration, but you're letting your personal experience override logic.
You've made a simple logical error: a study claiming that people who have goals can fend off depression does not imply that those with depression have it because they do not have goals. It means that some people who don't have goals, but do have depression, may remedy it by getting goals. But not everyone.
If the research above is resulting in psychiatrists becoming lazy, it's because they're making the same logical error you are making. So in that sense, you should avoid doing so, since the kind of error you are making is the very thing which leads to the behavior you've experienced.
The proper response (by you, and psychiatrists) is to conclude that trying to encourage goal formation in those with depression seems wise, and will help some, but many (like yourself) will not benefit. Nor should we invert causation and assume the reason people have depression is due to lack of goals, much like if we determined that eating a specific kind of food helped prevent cancer meant that those who for whatever reason didn't have that food in their diet were somehow causing their own cancer by neglecting to eat it.
> It means that some people who don't have goals, but do have depression, may remedy it by getting goals. But not everyone.
It really doesn't show this at all, you are misreading the study because the author of the article misrepresents it. Very few correlation studies turn into causation studies. Even when we have entire subfields dedicated to it. See amyloid beta.
Other possibilities "goals are protective against anxiety and depression but not changeable" "other factors increase goal driven behavior and protect against anxiety and depression" "goal driven behavior is protective but not curative of anxiety and depression" "goal driven behavior increases likelihood that individual gets treated for anxiety or depression"
Any of which would mean that increasing goal driven behavior would not help with anxiety or depression.
To me the article is not far from parent's reading. For instance these quotes:
> We wanted to understand what specific coping strategies would be helpful in reducing rates of depression, anxiety and panic attacks.
> Our findings suggest that people can improve their mental health by raising or maintaining high levels of tenacity, resilience and optimism,” she said. “Aspiring toward personal and career goals can make people feel like their lives have meaning. On the other hand, disengaging from striving toward those aims or having a cynical attitude can have high mental health costs.”
The second quote is really not far from presenting lack of perseverence or negativity as an active choice, putting the onus on the patient.
The second quote does not imply that all depressed people are such because they are lacking perseverance. There are several issues with this interpretation.
The first is that because something is on average true does not mean it is always true. There are cases where perseverance does not help depression. There are many where it does. On average it helps, which is the claim.
Next, it it is not fair to presume that because something helps, that it has a causal relationship with that thing. Most people feel less depressed (temporarily) if they take a dopamine agonist. This does not necessarily mean that their depression was caused by a lack of dopamine, only that dopamine helps. In the same way, focusing on goals will help a lot of depressed people. Influence does not imply causality.
And the last part of that statement about disengaging from goals and having a cynical attitude are also facts not conjecture. Negative thinking and disengaging from goal pursuit are linked to mood decline in virtually all people. This does not imply that people have full control over their thinking and goal pursuit or even that there aren't some people for whom such control is next to impossible.
As clinicians, we teach clients to work with what they have and make decisions that will help them. This study outlines some things that are typically helpful. It does not say that they will be helpful or possible for everyone.
I agree with your take as what the article is really meaning.
I think what trips me is that the article is not expliciting these caveats either. I fail to find a good analogy, perhaps it would be like explaining how sitting around is bad for your health to an audience including wheelchair users.
Sure, it wouldn’t be a false statement, but you’d try to address the elephant in the room somehow. I just wish people don’t get weird advice ideas for depressed people in their life reading the post.
That was my point. This study tells us nothing. The problem is not with people or the doctors, it is with these idiotic studies.
From the study:
"People who showed more goal persistence and optimism during the first assessment in the mid-1990s had greater reductions in depression, anxiety and panic disorders across the 18 years, according to the authors.
And throughout those years, people who began with fewer mental health problems showed more increased perseverance toward life goals and were better at focusing on the positive side of unfortunate events, said Zainal."
and they conclude with your inverted causation:
"Our findings suggest that people can improve their mental health by raising or maintaining high levels of tenacity, resilience and optimism,” she said. “Aspiring toward personal and career goals can make people feel like their lives have meaning. On the other hand, disengaging from striving toward those aims or having a cynical attitude can have high mental health costs.”
So people who are not depressed do not easily get depressed. Really? That is the ground breaking work? Re read that part, again and again, and tell me where my logic is wrong. They are saying correlation is causal.
Your emotion is clouding your ability to be reasonable about this. Saying that certain behavior can have treatment value does not imply that not doing that behavior was the cause.
If they said a heating pad could help me fix my muscle strain, does that mean they are saying that I caused a muscle strain by not using a heating pad? That's absurd of course.
They are saying that focusing on achievement of life goals (as opposed to focusing on "fixing" yourself) can have therapeutic value.
Why are you talking about my emotion? Because I said I have a mood disorder?
>If they said a heating pad could help me fix my muscle strain, does that mean they are saying that I caused a muscle strain by not using a heating pad? That's absurd of course.
If you look at the rest of this thread that is how everyone is interpreting it. read them and talk to them. I am not doing that, doctors do it.
What do you think is more reasonable, that your emotional commitments to this subject are distorting your read of the article, or that the American Psychological Association knows less than you do?
I just told you they were wrong about me during my 30 years of treatment. They thought I had a mood disorder but I had a metabolic disorder. so in this case, yes, they knew less than I did.
Your condition only affects 1 in 500,000 to 1 in 1 million newborns, whereas major depression has a 20% lifetime prevalence in the USA. For anxiety disorders, the rate is 30%.
Why do you have to be so rude? You didn't mention anything about PARTIAL GCH1 deficiency, and the ref you give is a from a single patient. The condition discussed in the article (DRD) affects one in a million people according to the NIH.
Given our recent experience with doctors killing people by putting them on ventilators when they could have put them on O2 I think blind faith in the APA is a bad idea, though I do generally see psychiatry and psychology as more professional than other fields of medicine.
Right, but this was a study conducted by the American Psychological Association, an organization that has literally nothing to do with the medical practices you spoke about.
The psychiatric equivalent is overprescribing antipsychotics because it makes people easier to manage. The general medical example was meant to be an impactful current example (though overprescription of antipsychotics is still happening).
No, he's interpreting the study perfectly well. The blame lies squarely with "trusted professionals" who can't think outside the box. Many psychiatrists commit the same fallacy you are describing, just in the other direction, which is what he's saying.
The more I am unfortunately exposed to this after catching ME/CFS the more I realise medicine has a huge professionalism problem. Maybe a better term is a religious problem. Anything they cant currently explain is the patients fault. Having chronic energy fatigue issues is just me being lazy apparently and the enormous crashes I get after exercise are me doing wrong. The hundreds of thousands of c19 patients that develop this condition will get the same thing.
To me it looks like most of them lack professional curiosity and certainly basic empathy. I lost all my respect for doctors over the 6 years based on how I have been treated.
Part of it is systemic though. Those that do have professional curiosity are unable to explore it due to constraints by insurance companies. Overall cost is the primary motive instead of quality of life. I imagine working in the medical industry is very disappointing for people that entered it with the intention of helping people.
Given I am in the UK alas that doesn't explain the issue. The USA is a bit of a unique unicorn in its for profit system but the world over there are these issues. I understand why the public is like that, a lot of people don't understand the scientific method but doctors have done all 3 of the sciences and then gone on for another 6 years of graduate and post graduate study.
The NHS has massive internal pressures on costs. It’s considered one of the most cost-effective health services in the world, but that’s because they will try to get away with doing the minimum they absolutely have to in order not to look negligent. Children and at-risk groups (the elderly, pregnant, etc) get a lot of care, everyone else is deprioritized and sent home with a bit of ibuprofen. I have experience of other health services on the continent and the comparison does not flatter the NHS.
Speaking as someone who has recovered from ME/CFS, stress and (lack of) goals seem to have been a big factor in causing me to develop the illness, and stress seems to be a major factor for other patients as well (according to both the research, and the experiences of patients themselves).
I don't see this as blaming myself, it's just how the brain works. Chronic stress has negative effects for all mammals. Take a look at forced swimming, visible burrow, or other stress experiments. It isn't the animal's fault that it has a negative reaction (in terms of cortisol, neurotransmitters, depression, anxiety, mental/physical fatigue, or whatever) to the stressful situation. The brain has evolved to generate these responses to stress, presumably as a survival tool to help prevent the even worse effects of chronic long-term stress. The one advantage we have as humans is that we have a certain amount of control in getting out of stressful situations.
Alas I am living that. I did my homework I have worked out what I want to do next and I am being told no. The tests I want they can't order as they are apparently too specialist for general practice and the drugs to find the issue via treatment are too far too off label for them to justify despite studies and clinical efficicacy from other countries. I just view that as a refusal to diagnose and treat me, no point putting it on me if you aren't then going to let me treat myself.
It is frankly absurd to put this onto the patient. It is all about their perceived Physchological basis of the disease, they will humour you on tests and some low harm drugs until you run out of stuff and hope you will finally see the light that CBT will help you.
If there is any test you should get is is a serum amino acid test.
I have done much of the foot work on ME/CFS. Start looking into aldehydes (malondialdehyde specifically) and the role they play. Also, if you can get your genetics from Ancestry it could help you understand yourself more.
To be fair, it is not the doctor’s fault entirely, it is an institutional problem.
We have far too few doctors per capita to have enough time to treat people. This is mostly because we have institutions set up that reduce the number of doctors that are output (e.g. we have about the same number of medical schools as 100 years ago).
tl;dr doctors have no time, there are lots of knock on effects to this.
> After I yelled at my doctors for years to look more deeply
This is the thing I hate most about dealing with doctors. As a child doctors failed to diagnose in me a condition so obvious that a friend of my mother, who works at an airport, was able to figure it out from a mere description. Still my mother had to get angry with the doctor before he would perform a simple blood test for it!
Like in any profession, most of them suck at their job. That wouldn't be such a big deal except that the system in the US is set up to make it absurdly difficult and ludicrously expensive to shop around.
And, once you are diagnosed with a mood disorder they will not look at anything else. Anything other symptom arises from "my mood disorder". Skin issues, hyperlipidemia, gut issues, pain, etc...all in my head.
In medical school, many doctors learn the saying, “When you hear hoof beats, think horses, not zebras.” Most physicians are taught to focus on the likeliest possibilities when making a diagnosis, not the unusual ones.
However, it seems that some physicians oversimplify diagnosis so that _only_ the likeliest scenarios are considered. It's also an opportunity for subjective biases to influence an individual doctors definition of "likely."
I "only" had a bad situational depression but when I was at the bottom it was clear that nothing normal, pep talk etc was connected to my reality. And even long after that it was infuriating to be talked down by people with 'lazy' innuendos.
Yet ... I myself realize that in my brain there's a little 'will' part that you can focus on which kinda resonnated with the self part of depression and how you may (in time) give it a push to move away from the depressive state faster.
Sorry if it annoys you, I'm mostly trying to share my experience. Do the best you can in you context. Best wishes.
"Just get a hobby","Go outside more","Set better goals","Pray more","Eat Better","Just adjust your mindset","Just work harder","Make your bed","Read a book","Try meditation","Take a nap","Drink more water","Doubt your doubt", and on, and on, and on, and on, and on, and on, ...
Out of curiosity, what country offers disability benefits for these conditions?
This is for me a (as a fellow sufferer of some of these conditions, who has never received any state support and doesn't even have health insurance) an extremely shaky moral ground.
Because 95% of the homeless population and drug addicts are clinically diagnosable of most of these conditions under DSM IV definitions. And almost none of them receive anything.
I am in the U.S. and I am lucky because I am white and my OCD kept me from using any drugs to cope. But I was hospitalized several times and had a few suicide attempts, plus my family history. Those are all big factors in getting disability.
If you are homeless and do not have an address there is zero chance to get disability. That is why we should house them first without any qualifications. Or maybe they justneed to set better goals. :)
Legally, no. Functionally, yes. Even though they no longer mail checks you need a bank account as well. And then the issue with getting in contact with you.
There is only wealth in this country because we treat the most vulnerable like garbage.
I would guess most European welfare states offer disability benefits for severe depression. For example Finland has disability pension system for people who are verified by a doctor unable to work anymore. Severe depression is an acceptable condition for this benefit.
> So what is this article saying? Me and my family just do not have perseverance?
I think it's more likely that if you're not depressed, chronically anxious or having panic attacks, you'll find it far easier to muster some perseverance.
No, it is saying that having perseverence and working towards goals helps:
“Our findings suggest that people can improve their mental health by raising or maintaining high levels of tenacity, resilience and optimism,” she said. “Aspiring toward personal and career goals can make people feel like their lives have meaning. On the other hand, disengaging from striving toward those aims or having a cynical attitude can have high mental health costs.”
That seems unlikely, since they didn't find any correlation between baseline depression and future goals, only between baseline goals and future depression.
"Greater within-subject increased goal persistence (but not positive reappraisal or self-mastery) led to
larger future declines in disorder counts. However, within-subject change in disorder counts did not
substantially influence future change in each cognitive or behavioral strategy"
They were not studying people with depression and anxiety, it was a general population. So this might work for people in general, but not with people with depression and anxiety.
Participants were 3,294 community-dwelling adults ages 45.62 years
> they finally found that it was not that I did not have goals, but that I needed a low protein diet and some medications that a psychiatrist could not give me, and now I am doing better.
I think that's a problem with the influence of psychology within psychiatry? There is little ability to distinguish organic disorders and the endogenous vs. exogenous question only really gets resolved with respect to whole diagnoses, less common to distinguish w.r.t. an individual.
> some medications that a psychiatrist could not give me
Curious, were these medications for the symptoms you mentioned in general (Depression, Anxiety, Panic Disorders), or specific to the genetic disorder that caused those symptoms?
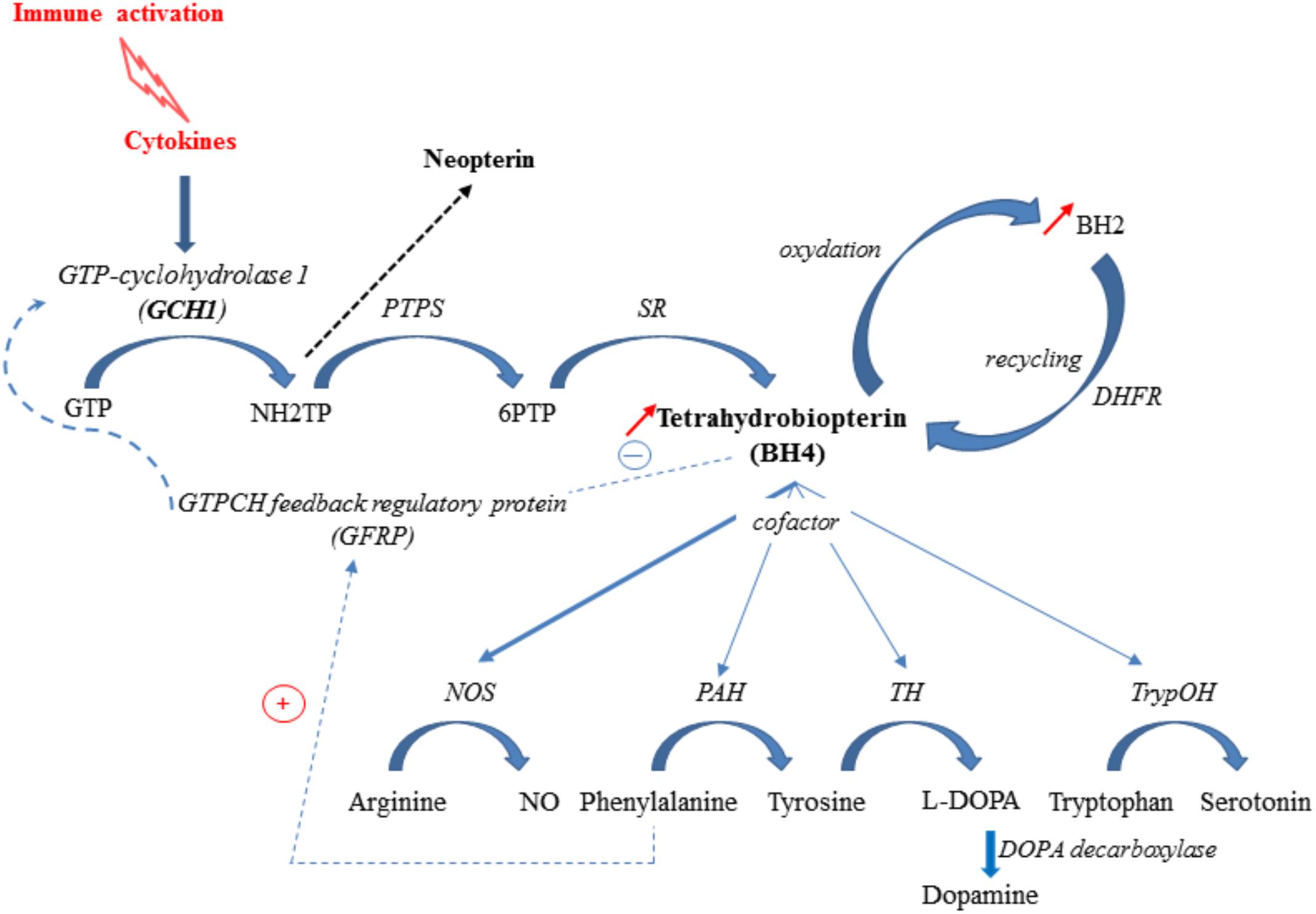
Since we do not make enough BH4 (tetrahydrobiopterin) with this enzyme deficiency we cannot metabolize the amino acids needed to make serotonin, dopamine, and Nirtic Oxide. And then some of these amino acids turn into trace amines that act like meth.
The deficiency causes problems with amino acid metabolism, which themselves mess up the brain.
The depression was a mere symptom of the underlying disease. When you read the DSM, you realize there are no mental illnesses, just syndromes: sets of signs and symptoms. Except in select few cases, the pathophysiology is unknown.
Protein is split into amino acids and then recombined into proteins inside body. The splitting process and recombination process need glucose in blood and, effectively, drain glucose from blood.
In my experience, some of the amino acid sport drinks can drain glucose from blood to the point where I had clear signs of very low glucose levels, including restlessness and shaking limbs.
The glucose level may affect mood and has other interesting effects.
If you look at what carbs, fats and proteins do with you mood, I think you will see that carbs make one relaxed (see relation between carbs and orexin), fats make one jolly (due to endocannabioids) and proteins make one awake (draining carbs from blood, mainly).
{kind=link}
So what is this article saying? Me and my family just do not have perseverance? That we lack the "will" not to be depressed and anxious? That I just need to "Aspir[e] toward personal and career goals"? HA!
No, it's not true. You see, they found we all have a genetic disorder (GCH1 Deficiency). After I yelled at my doctors for years to look more deeply they finally found that it was not that I did not have goals, but that I needed a low protein diet and some medications that a psychiatrist could not give me, and now I am doing better. Now I can have goals.
So while this article might be true for some people with situational depression, I hate these studies because people always said crap like this to me. I was "lazy" and just needed a hobby, and on and on. They psychiatric association does not recognize, still, that mood disorders can be caused by metabolic issues. When they say I do not have enough serotonin and I ask them why they looked at me like they were in Psych 101. And these articles make psychiatrists lazy, putting all the effort on the patient while they sit back and collect check after check.