For a week I've been wondering about Germany's numbers. Maybe they are doing something wrong, or maybe it is China and Italy that are giving us bad data.
Roche’s Cobas 8800 can do roughly ~4100 tests per day and this is a massive full-room setup.
Many other RT-PCR capable machines exist out there (800 is the total number in Europe cumulative) but this assumes an efficient point-of test > courier > lab > results process which many countries simply lack.
However, this assumes the current surge deaths are 100% SARS-Cov2 confirmed infections.
They aren’t. At least not 100%
Assumption can be made “atypical, bad flu season” but safer bet is on “newly discovered virus out of China that did x and y and z damage over there.”
While both theories are just that, theories. There is no empirical data which PROVES x-cases and y-surge is directly related to a confirmed SARS-Cov2 pathogen confirmed by RT-PCR and antibody test.
The Italian data is wrong period. Why or how is another debate.
All dead patients were tested and they were positive. The Italian ISS is reporting that those patients went full ICU with the most common symptoms associated with Covid-19, notably respiratory failure, then "danno renale acuto", "danno miocardico acuto" and "dovrainfezione", which I'm not going to translate for you, and this is happening regardless of their pre-existing conditions. There's no easy assumption except yours. Stop blaming italian professionals and I invite you to visit our government websites for the details, for which I'm not going to provide a link for you. Also, there is no guessing game as to who is affected by the virus. Again, you need not to mix your prejudice against Italians with the emergency we are having.
Italians are most likely counting most if not all deaths as SARS-Cov2 deaths.
1) A large amount of the elderly are going to hospitals because of pre-existing conditions that might be flaring up or presenting as they normally do. They enter the clinic > get complications > get marked down as dying from SARS-Cov2. And/or they acquire hospital acquired pneumonia (HAP).
2) I’ve read the ISS report cover to cover and yes, nearly ALL deaths are due to 1) age greater than 70, 2) 75% showing 2 (two) or more per-existing conditions with a staggering 99% showing 1 (one) or more pre-existing conditions. Let’s not forget the above comment (HAP or other hospital acquired infections from SARS-Cov2, Influenza, whatever).
3) Seeing a death count YOY would be beneficial here indeed.
I don’t think ANYBODY will be able to answer my initial question here.
There is NO WAY in hell the Italians have tested over 200,000 patients for SARS-Cov2 in a matter of 2-3 weeks due to:
1) such capacity simply does not exist
2) Italians have been under quarantine and when they weren’t they were drinking coffee and not lining up for tests.
3) the time of test > result trajectory > reported data is impossible
4) such high throughout testing capacity simply does not exist
Also in Italy, unlike what happens in other countries, all deceased people positive to the test are classified as "Covid deaths", regardless of the simultaneous presence of other serious diseases.
Germany is able to conduct more than 160,000 tests per week. I do not know the numbers for Italy, but why shouldn't they be able to reach that number over 2-3 weeks?
Apples to oranges. Can not compare Italy with Germany.
Germans are willingly being tested, there process, order, proactive testing. In Italy everyone is 1) quarantined for the past 2 weeks and 2) didn’t even give a crap about this prior to the quarantine.
Italy is triaging, out of hospital space, vastly over estimating numbers, and probably using models with some accuracy to report their numbers. Unless someone can PROVE this otherwise.
Their death rate is what it is due to a very elderly population, with 2 or more co-morbidities, in understaffed and overwhelmed hospitals full of chaos, and infection.
If the average number of cases in some small area (e.g. a block or blocks of buildings, a part of town, a town) is e.g. two patients with symptoms X per MONTH, and the symptoms include FEVER and not being able to breath, i.e. something people can't just make up and can be easily measured, and THEN you get a patient from a block of buildings with symptoms X and THEN you test him and get a positive result and THEN you get ten more people from there with symptoms X, AND in the same small are some people have the same symptoms and are in such a bad condition that they need to be connected to the MACHINES and some DIE, you can be very sure it's a virus which never existed among the humans before generating these symptoms.
Otherwise, it would have to be some OTHER virus not known to humanity appearing at the same time, behaving unlike the viruses we know and watch every year, magically appearing exactly in the community where you verified the existence of the one for which you test.
It very much is. When you are limited in every way you have make some cuts. This is just the cut that says that it is probably covid if it is not flu and they are from an area with test confirmed cases. And in by far most cases it is going to be correct. Probably as correct as the current test for covid.
So 200,000+ people under mandatory lockdown went to a clinic (not a drive through test, a physical clinic), lined up and waited to get tested for Influenza which was assumed to be SARS-Cov2?
Or maybe Italy tested 200,000+ samples with RT-PCR technology with machines and labs and tests / swabs they don’t have?
Not trying at all to spin conspiracy theories here but these numbers simply do not add up.
As a corollary: there are a myriad of infections that can present as fever and cough: rhinoviruses, influenza, bronchial infections, gastroenteritis, auto immune flare ups, sinusitis and season allergies, the list goes on.
They can just test for Covid-19 antibodies. It's not really reliable, but it is much faster than the genetic tests and should quickly discriminate between Covid and the common flu.
Italians are triaging, so they have to quickly sort the cases. They have to sacrifice precision and allow for some false positives.
This is very much a game of assumptions and a game of cutting corners at this point. It's wartime. The hospitals near me are literally using pieces of cotton, cut shirts, hand-sewn layers, instead of regulation-required certified N95 masks.
Right. One issue we’re having globally is that we simply cannot get an accurate fatality rate.
We’re only seeing the sickest, most critical patients and the most overwhelmed hospital systems in cities.
I think MOST patients being tested in hotspots like Lombardy are those who are already at the hospital, and if you’re at the hospital you’re not in good shape.
Probably tons of positive cases at home with a fever, or mild symptoms or no symptoms.
And of course, tons of people who are not tested and probably never will be. Totally asymptomatic.
We can’t get an accurate fatality rate without these “infected but asymptomatic” cases.
Didn’t an Italian doctor do a small study showing 98% asymptomatic positive cases?
Germany currently looks to be an interesting case. As of CNN this morning, they have 13,957 cases confirmed, and 31 deaths. The deaths may of course crank up to a "normal" level, but I wonder if it's possible that they are testing many more people and getting a more accurate view.
(of course, this comment will probably age poorly)
Sorry about the paywall. If you search for it via google and click it from there that's how I found it (and why I didn't realize it was paywall)
Basic summary: Too Early to tell. But Germany is doing 160,000 tests/week, which is more than lots of countries. They may be getting a more complete picture of who is all infected.
We have enough data from closed experiments (Diamond Princess) to say that COVID sends 5% or more to the ICU. That’s the number that matters right now, not CFR. Fatality rate itself is much more dependent on whether the ICU beds are full (Italy, Iran) than anything else. Unfortunately, beds are about to be full in several US cities.
But that's not reliable either. Average age on the Diamond Princess was 58. With 1/3 being over 70. Average age in the US is 38, with 15.2% being over 65.
Given that age is a very large component here, I don't think you can extrapolate data from the Diamond Princess to the general population.
My source is an interview in the first German state TV station (ARD). I am sorry that I can't provide you with an English source. If you understand German, please watch https://youtu.be/IHF0IDtW6LA?t=882 from minute 14:42.
Probably tens of thousands of undiagnosed, asymptomatic.
Aka super carriers.
The virus is smart and has evolved from an evolutionary standpoint. Infect younger and asymptomatic patients with the goal of spreading and infecting as many as possible. Eventually, the more infected, the more that will die. The young are just carrier pigeons and don’t even know it.
> The virus is smart and has evolved from an evolutionary standpoint. Infect younger and asymptomatic patients with the goal of spreading and infecting as many as possible.
I think you are giving a bit too much agency to the virus. It has evolved in such a way that optimises for further spreading for sure, but I do not think it has a sneaky strategy to use young people as attack vectors.
What's more likely is that it has evolved to replicate and spread within the human population, while not acting so fast as to kill most people. The problem is that replicating at a rate that doesn't kill most people will kill some of the oldest and sickest within a population.
Another important insight is that Viruses, and germs in general, try to evolve and adapt inside the host. They don’t gain if they end up killing the host because that ends them too.
Not to sound apocalyptic but I think their holy grail is something like what the machines do to humans in the movie Matrix
> Another important insight is that Viruses, and germs in general, try to evolve and adapt inside the host.
That assumption has no basis at all. Evolutionary pressures don't happen due to a intentional guidance from the evolving species. Individuals mutate by chance and replicate as they can. That's it.
You're making a mountain out of a mole hill. The virus spreads as it's possible, and those who carry the virus experience the infection differently depending on some traits.
- Mean age of 79.5 sheds light on Italy’s extremely high fatality rates; in essence, it’s the (very) elderly that are dying due to complications from viral pneumonia. Which begs the next question...
Why are they overwhelmingly treating patients with antibiotics in cases of viral pneumonia and not antivirals (Remdesivir)/ chloroquine?
Sure, these are “experimental” therapies but decent data out of China/South Korea shows these therapies work. Perhaps they found out too late?
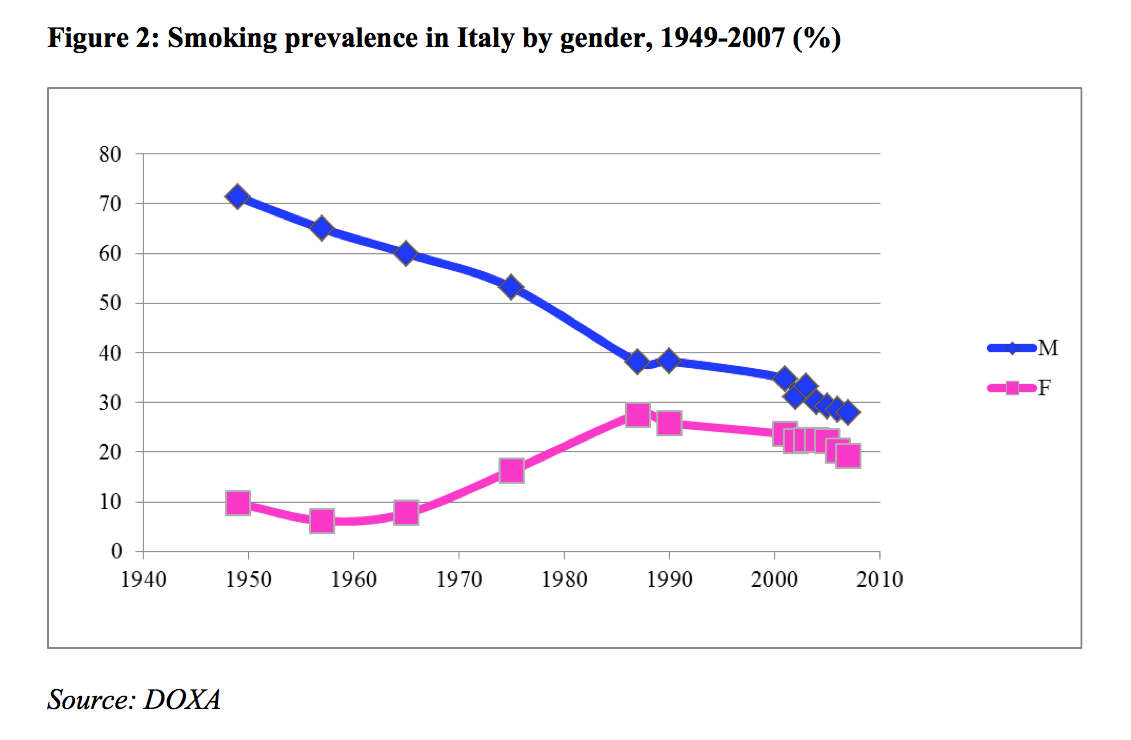
- The younger fatalities (17) show multiple, serious co-morbidities and smoking is not listed; an assumption can be made a fair amount of these younger patients smoke. But again, an assumption.
- Almost 50% of patients showed 3 or more co-morbidities - this is high and important to note. 25% of patients showed 2 co-morbidities. Roughly 75% of patients had 2 or more co-morbidities (!).
- Sample size (2003) is good given their current 3,500 fatality numbers.
Not a medical doctor but a few things I’m struggling to figure out:
- How did so many elderly get infected? Did the disease simply spread in close quarters where many elderly live? Elderly folks aren’t necessarily out and about drinking espresso and touching surfaces yet alone having younger asymptomatic carriers cough on them.
I wonder if Italy is similar to a Kirkland, Washington situation. High density of elderly folks spreading infection.
It’s obvious that SARS-Cov-2 is highly, highly contagious but it’s interesting how we’re seeing these somewhat “bomb” explosions of infection: Wuhan > Daegu > Kirkland > Lombardy > NYC next.
Sure, quarantine works but the rate of new infection stays rather localized and then just annihilates everyone around it.
Perhaps it’s a viral load issue; viral load increases exponentially the more we have infected. Why you see doctors and nurses infected / critical and dying even with full PPE.
Let’s hope the Italians figure out a way to get this curve to fall of ASAP. Hoping they have a similar effect to Wuhan’s curve and just drop down rather than flatten.
There’s truth to this and perhaps I jumped to an invalid American based assumption, stupid given that I’m European.
In Europe, the elderly are out and about, walking, sitting at parks, drinking coffee, the works. They’re actually still doing this as we speak in countries, from what friends and family tell me. Go figure.
However, even if they are in cafes, grocery stores, parks - the numbers are still very high.
This virus is either incredibly efficient and contagious (spread by totally asymptotic carrier pigeon patients > elderly) and/or it’s been there for a long time. Months.
If my experience with 'southern' cultures is anything to go by, the amount of interaction between young and old people probably plays a huge role.
For comparison, I live in NL and for me and the vast majority of my 20-30-something friends, visiting grandparents is relatively rare. For many of us even visiting parents is a 'once every x months' kind of thing.
On the other hand, when I lived around the mediterranean, not only was it expected to regularly interact with parents and grandparents, but it was often the case that they lived together, or at least close by.
Perhaps the 'quarantining'/neglect of the elderly in Northern-Europe that I've often criticised as inhumane is actually saving them in this particular situation.
> This virus is either incredibly efficient and contagious (spread by totally asymptotic carrier pigeon patients > elderly) and/or it’s been there for a long time. Months.
It's incredibly contagious. Infection rate doubles every 2.5 days.
> Why are they overwhelmingly treating patients with antibiotics in cases of viral pneumonia and not antivirals (Remdesivir)/ chloroquine?
My guess is that they try to avoid an additional bacterial super infection with antibiotics. Also these antivirals can be dangerous to (very) old people. I think because of liver malfunctions. But take all I say with a grain of salt.. this is all stuff in the back off my head that I remember vaguely from my father (a doctor).
My understanding is that the virus greatly hinders your immune response in the lungs and that opens the door to microbial infections. This is what causes the severe pneumonias that kill people. Kurzgesagt did a nice video explaining this: https://www.youtube.com/watch?v=BtN-goy9VOY
> The figure 5 shows, for the patients who died positive COVID-19, the median time in days, who spend from onset of symptoms to death (8 days), from onset of symptoms to hospitalization (4 days) and from hospitalization to death (4 days).
At this point, we know the elderly and people with pre-existing conditions are dying fast; it is also not unreasonable to think they're more vulnerable overall.
But not enough time has passed to say yet whether younger people without pre-existing conditions are not particularly susceptible or are just a little less susceptible but take longer to succumb. If the statistics are a week for someone over 65, from onset to death, and a month for someone under 40 w/o pre-existing conditions, it's going to skew the hell out of the statistics this early in the outbreak.
> How did so many elderly get infected? Did the disease simply spread in close quarters where many elderly live? Elderly folks aren’t necessarily out and about drinking espresso and touching surfaces yet alone having younger asymptomatic carriers cough on them.
Ha. Italians in N. Italy often living multigeneration in close quarters. Spanish and italians, men and women, ritually kiss on the cheeks as a greeting. Brits and Germans don't so much.
Italians are very social to an old age and live longer than many nations.
> How did so many elderly get infected? Did the disease simply spread in close quarters where many elderly live? Elderly folks aren’t necessarily out and about drinking espresso and touching surfaces yet alone having younger asymptomatic carriers cough on them.
I was wondering the same thing, but judging by my own country crowds of elderly people is a thing. For example they do not use technology as much as others and tend to concentrate in places that provide alternative means to function without technology.
Another assumption is that touching surfaces is not how the virus spreads. Being within a few meters of carriers, not necessarily coughing, just talking and breathing, is how people catch it. And since masks are not available and dumb propaganda discourages people from using even a piece of clothing to protect them from inhaling droplets, people catch the virus so easily.
> Why are they overwhelmingly treating patients with antibiotics in cases of viral pneumonia and not antivirals (Remdesivir)/ chloroquine?
Because a bunch of these patients are people with suspected, not confirmed, covid-19 and so they're treating pneumonia which they think is probably bacterial but possibly viral.
Also, they were thinking that covid-19 in already vulnerable people was damaging the lungs and making bacterial pneumonia much more likely, so they were treating preventatively.
> yet alone having younger asymptomatic carriers cough on them.
Droplets in the air are one route of transmission, but there are others. It's likely that most people are not infected via this route, but via fomites. Infected people cough onto a surface, and later someone touches that surface and then their face.
> How does the virus get from their face into the lungs in enough quantity to infect them?
They're already infected. I don't understand the question. Are you asking how the virus replicates? It's a strand of RNA that takes over human cell replication. It binds to ACE2, which is how it targets lungs. https://blogs.plos.org/dnascience/2020/02/20/covid-19-vaccin...
It's unusual for people in public places to be coughed on. I can't think of it happening to me in the past 5 years.
Healthcare professionals wear masks (and goggles, and protective clothing, and sometimes gloves) because their work involves close contact with ill people who are coughing over them.
On antibiotics, aside from secondary infections, there’s a paper out talking about azithromycin:
“Our preliminary results also suggest a synergistic effect of the combination of hydroxychloroquine and azithromycin. Azithromycin has been shown to be active in vitro against Zika and Ebola viruses [20-22] and to prevent severe respiratory tract infections when administrated to patients suffering viral infection [23].”
Not sure of they used azithromycin but would’ve been good to see that verified.
It is everywhere. The 'pockets' you think you are seeing are an artifact of exponential growth. When infection rate doubles every 2.5 days, the incubation time is 5-14 days and it take 3-4 weeks to die the first 4 weeks look harmless. But by then it is already well out of control.
We all want to live long, and people now often live till 80+, but when a person 80+ years old dies does it make sense to search for a cause of the death? My grandmother died last year from pneumonia. She was 89, which is way above the average life expectancy. Any small infection can kill a person at this age. Is there a statistics that shows the mortality rate in Italy before the pandemic.
{kind=link}
Italy is counting ALL deaths as Covid deaths.
Their Covid numbers are simply incorrect.